Ovulation is the reproductive process in which a mature egg (ovum) is released from the ovarian follicle into the fallopian tube, marking the fertile window of the menstrual cycle. Ovulation typically occurs approximately 14 days before the start of the next menstrual period and is triggered by a surge in luteinizing hormone (LH), representing the culmination of complex hormonal interactions that prepare the female reproductive system for potential fertilization. At the population level, ovulation occurs in approximately 400-500 cycles throughout a woman’s reproductive lifespan, with timing and regularity influenced by factors including age, health status, stress levels, and individual hormonal patterns.
Ovulation
| |
|---|---|
| Category | Reproductive Health, Gynecology, Endocrinology |
| Research Fields | Reproductive Endocrinology, Gynecology, Fertility Medicine, Chronobiology |
| Also known as: | Egg release, follicular rupture, ovum expulsion |
| Pronunciation: | ah-vyuh-LAY-shuhn |
| Typical cycle day: | Day 14 (in 28-day cycle) |
| Fertile window: | 5 days before to 1 day after ovulation |
| LH surge duration: | 12-36 hours before ovulation |
| Egg viability: | 12-24 hours post-ovulation |
| Lifetime ovulations: | ~400-500 total cycles |
| Sources: | ACOG, Human Reproduction, StatPearls, Fertility and Sterility |

Scientific research demonstrates that ovulation is precisely orchestrated by the hypothalamic-pituitary-ovarian axis, with follicle-stimulating hormone (FSH) promoting follicle development and the LH surge triggering ovulation within 12-36 hours. The fertile window extends approximately 5 days before ovulation through 1 day after, during which conception is most likely to occur. Studies show that only 10-15% of women ovulate exactly on day 14 of their cycle, with normal ovulation occurring anywhere from day 11-21 in regular cycles.
Ovulation disorders affect approximately 25% of couples experiencing infertility, making understanding ovulation patterns crucial for both achieving and preventing pregnancy. Comprehensive ovulation awareness encompasses knowledge of cycle tracking methods, ovulation signs and symptoms, factors affecting timing, and the relationship between ovulation and fertility optimization.
History
Ancient Understanding
Ancient civilizations recognized connections between menstruation and fertility, though the specific process of ovulation was not understood. Greek physician Hippocrates (460-370 BCE) wrote about female reproductive cycles, while ancient Chinese and Indian medical texts documented relationships between lunar cycles and female fertility.
Medieval and Renaissance Observations
Medieval Islamic physicians including Al-Razi and Ibn Sina made important observations about menstrual cycles and fertility timing. Renaissance anatomists began detailed studies of female reproductive anatomy, laying groundwork for understanding ovarian function.
17th Century: First Ovarian Observations
Dutch physician Regnier de Graaf (1641-1673) provided the first detailed descriptions of ovarian follicles, now called Graafian follicles. His work “De Mulierum Organis Generationi Inservientibus” documented ovarian structures and their role in reproduction.
1827: Discovery of the Mammalian Egg
Karl Ernst von Baer discovered the mammalian ovum, providing the first direct evidence of egg cells in mammals. This discovery revolutionized understanding of female reproductive biology and laid the foundation for comprehending ovulation.
1930s: Hormonal Discovery
The discovery of reproductive hormones including estrogen, progesterone, FSH, and LH revealed the complex endocrine control of ovulation. This period established the hormonal basis of the menstrual cycle and ovulation timing.
1950s-1960s: LH Surge Identification
Researchers identified the luteinizing hormone surge as the trigger for ovulation, establishing the precise hormonal mechanism that releases the mature egg from the follicle. This discovery enabled development of ovulation prediction methods.
1970s-1980s: Fertility Awareness
Development of fertility awareness methods and ovulation prediction tools allowed women to identify their fertile periods accurately. Basal body temperature charting and cervical mucus observation became established natural family planning techniques.
1990s-Present: Modern Monitoring
Advanced reproductive technologies including ultrasound monitoring, hormone assays, and digital ovulation predictors have refined understanding of ovulation timing and enabled precise fertility management for both achieving and avoiding pregnancy.
Biological Mechanisms
Hormonal Cascade
Ovulation is controlled by the hypothalamic-pituitary-ovarian axis through a precisely timed hormonal cascade. The hypothalamus releases GnRH (gonadotropin-releasing hormone), stimulating the pituitary to produce FSH and LH. FSH promotes follicle development, while rising estrogen levels trigger the LH surge that causes ovulation.
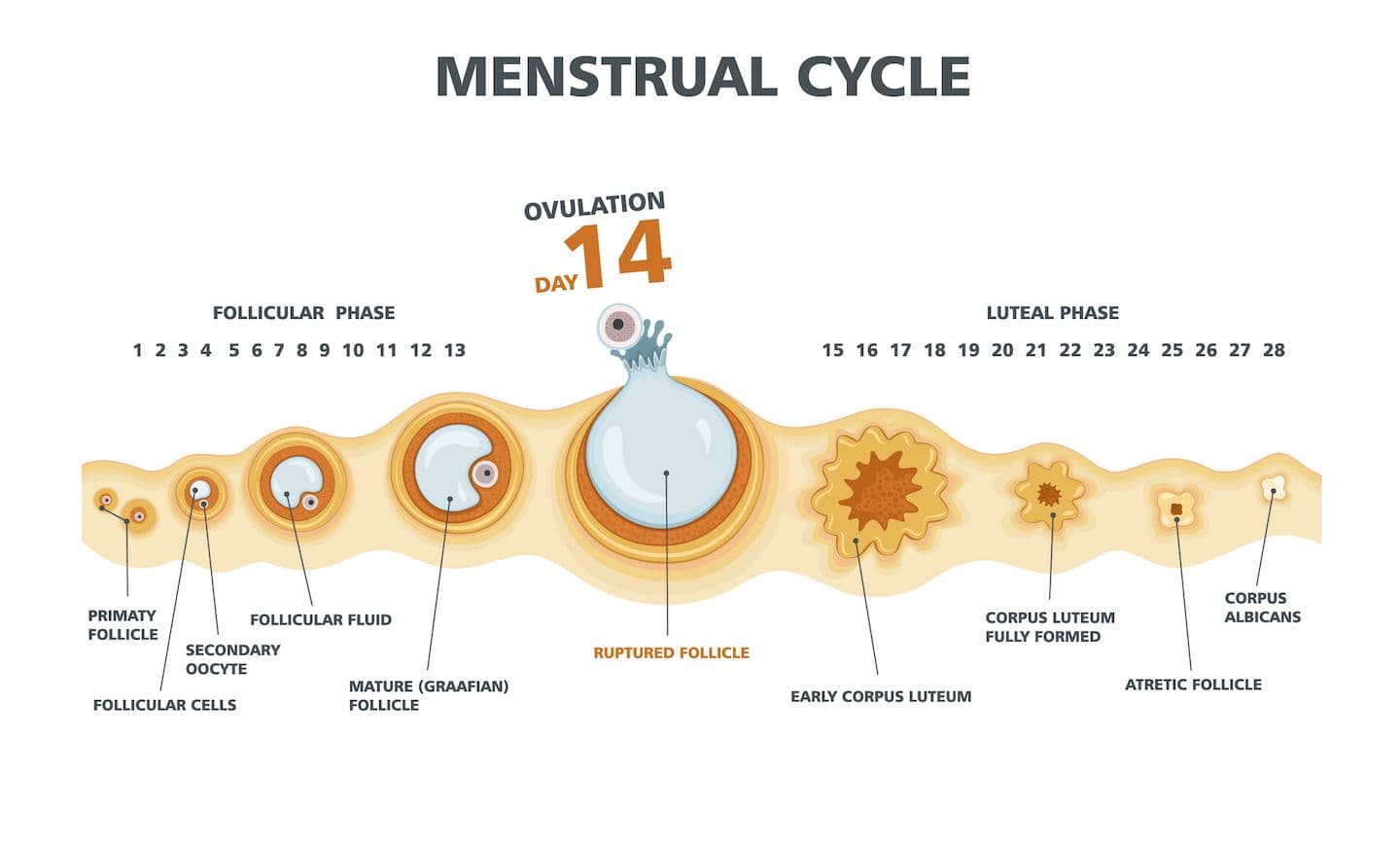
Follicular Development
Each menstrual cycle begins with recruitment of multiple primordial follicles, though typically only one becomes dominant and continues to maturity. The dominant follicle grows from 2-3mm to 18-25mm in diameter, with the mature egg surrounded by cumulus cells that support fertilization.
Ovulation Process
The LH surge causes rapid follicle expansion, enzymatic breakdown of the follicle wall, and release of the egg along with surrounding cumulus cells. The process takes approximately 12-36 hours from LH surge onset to actual egg release, creating the ovulation window.
Corpus Luteum Formation
After ovulation, the ruptured follicle transforms into the corpus luteum, which produces progesterone to support potential pregnancy. If fertilization doesn’t occur, the corpus luteum degenerates after 10-14 days, leading to menstruation and beginning of a new cycle.
Ovulation Signs and Symptoms
Physical Symptoms
Many women experience physical signs around ovulation including mittelschmerz (ovulation pain), breast tenderness, mild bloating, and increased energy. Mittelschmerz affects approximately 20% of women and can alternate between ovaries each cycle, providing a natural ovulation indicator.
Cervical Mucus Changes
Cervical mucus undergoes dramatic changes throughout the cycle, becoming clear, stretchy, and slippery around ovulation – often described as having an “egg white” consistency. This fertile cervical mucus facilitates sperm transport and survival, providing an important fertility sign.
Basal Body Temperature
Basal body temperature (BBT) rises 0.2-0.5°C (0.4-1.0°F) after ovulation due to progesterone’s thermogenic effect. While BBT confirms ovulation has occurred, it doesn’t predict ovulation timing, making it more useful for retrospective cycle analysis than conception timing.
Hormonal Fluctuations
The LH surge can be detected in urine 12-36 hours before ovulation using over-the-counter ovulation predictor kits. Some women also experience mood changes, increased libido, or enhanced sense of smell around ovulation due to hormonal fluctuations.
Cycle Timing and Variability
Normal Cycle Patterns
While the “textbook” 28-day cycle with day 14 ovulation is commonly referenced, normal cycles range from 21-35 days with ovulation occurring 12-16 days before the next period. The luteal phase (post-ovulation) is more consistent at 10-16 days, while the follicular phase shows greater variation.
Individual Variation
Ovulation timing varies significantly among women and can vary within the same woman across different cycles. Studies show that only 10% of women consistently ovulate on the same cycle day, highlighting the importance of cycle tracking for accurate fertility awareness.
Age-Related Changes
Ovulation patterns change throughout the reproductive lifespan. Adolescents often have irregular ovulation initially, adults typically develop predictable patterns, and perimenopause brings increasing irregularity as ovarian function declines with age.
Cycle Length Determinants
Factors influencing cycle length and ovulation timing include stress levels, weight changes, exercise intensity, illness, travel, and hormonal fluctuations. Understanding ovulation variability helps women recognize normal fluctuations versus concerning changes requiring medical evaluation.
Fertility Window and Conception
Sperm Survival
Sperm can survive in fertile cervical mucus for up to 5 days, creating a fertile window that begins several days before ovulation. This survival depends on optimal cervical mucus quality and vaginal pH, which change throughout the cycle to support or inhibit sperm function.
Egg Viability
Once released, eggs remain viable for fertilization for approximately 12-24 hours. This short window means that timing intercourse in the days leading up to ovulation is generally more effective for conception than waiting until after ovulation occurs.
Optimal Conception Timing
Research indicates that conception is most likely when intercourse occurs in the 3 days leading up to ovulation, with the day before ovulation showing the highest conception rates. Daily or every-other-day intercourse during the fertile window optimizes conception chances.
Fertilization Process
Fertilization typically occurs in the fallopian tube within hours of ovulation. The fertilized egg then travels to the uterus over 6-7 days, with implantation occurring 6-12 days after ovulation if conception is successful.
Ovulation Disorders
Anovulation
Anovulation (absence of ovulation) can be chronic or intermittent, affecting 6-15% of reproductive-aged women. Causes include polycystic ovary syndrome (PCOS), hypothalamic dysfunction, premature ovarian insufficiency, and stress-related hormonal disruption.
Oligovulation
Oligovulation (infrequent ovulation) results in cycles longer than 35 days and reduced annual fertility opportunities. Common causes include PCOS, thyroid disorders, hyperprolactinemia, and significant weight changes affecting hormonal balance.
Luteal Phase Defects
Luteal phase defects involve inadequate progesterone production after ovulation, potentially impairing embryo implantation. While controversial as a distinct diagnosis, short luteal phases (less than 10 days) may indicate underlying ovulatory dysfunction.
Ovulatory Dysfunction Diagnosis
Diagnosing ovulation disorders involves tracking menstrual patterns, measuring hormones (LH, FSH, progesterone, prolactin, thyroid), and sometimes ultrasound monitoring of follicle development. Treatment depends on underlying causes and reproductive goals.
Tracking and Prediction Methods
Fertility Awareness Methods
Traditional fertility awareness methods include basal body temperature charting, cervical mucus observation, and calendar tracking. When used correctly, these methods can be 95-99% effective for identifying fertile periods, though they require training and consistent application.
Ovulation Predictor Kits
Over-the-counter ovulation predictor kits detect the LH surge in urine, providing 12-36 hours advance notice of ovulation. Digital tests offer clearer results than line tests, while some advanced kits also measure estrogen to extend the fertile window prediction.
Digital Fertility Monitors
Advanced fertility monitors track multiple hormones (LH, estrogen) and may incorporate additional data like temperature or heart rate. These devices can identify up to 6 fertile days per cycle and provide personalized cycle learning over time.
Mobile Apps and Wearables
Smartphone apps and wearable devices increasingly offer ovulation tracking through various inputs including cycle history, symptoms, temperature, and sometimes hormone data. While convenient, accuracy varies significantly among different platforms and approaches.
Factors Affecting Ovulation
Lifestyle Factors
Diet, exercise, sleep patterns, and stress management significantly influence ovulation regularity. Extreme caloric restriction, excessive exercise, or chronic stress can disrupt the hypothalamic-pituitary-ovarian axis and delay or prevent ovulation.
Body Weight
Both underweight (BMI <18.5) and overweight (BMI >25) conditions can affect ovulation through hormonal imbalances. Obesity increases insulin resistance and androgen production, while underweight status may suppress reproductive hormones entirely.
Medical Conditions
Conditions affecting ovulation include PCOS, thyroid disorders, diabetes, autoimmune diseases, and eating disorders. Many medications including antidepressants, antipsychotics, and some pain medications can also disrupt ovulatory function.
Environmental Factors
Environmental toxins, endocrine disruptors, shift work, and circadian rhythm disruption can affect ovulation timing and quality. Environmental influences on ovulation are increasingly recognized as important factors in reproductive health.
Ovulation Induction and Enhancement
Lifestyle Interventions
First-line approaches for optimizing ovulation include achieving healthy body weight, regular moderate exercise, stress reduction, adequate sleep, and nutritional optimization. These interventions can restore ovulation in many women with mild ovulatory dysfunction.
Ovulation Induction Medications
Medical ovulation induction includes clomiphene citrate (Clomid), letrozole, and gonadotropin injections. These medications stimulate follicle development and ovulation in women with anovulation or oligovulation, though they require medical monitoring for safety and effectiveness.
Metformin and Insulin Sensitizers
For women with PCOS and insulin resistance, metformin and other insulin sensitizers can restore ovulation by improving metabolic function. These medications work synergistically with lifestyle modifications and ovulation induction agents.
Surgical Interventions
Laparoscopic ovarian drilling (LOD) can restore ovulation in some women with PCOS who don’t respond to medications. This minimally invasive procedure reduces ovarian androgen production and can restore spontaneous ovulation cycles.
Ovulation and Natural Family Planning
Fertility Awareness-Based Methods
Natural family planning relies on identifying fertile and infertile phases of the menstrual cycle to either achieve or avoid pregnancy. Effective methods require understanding multiple fertility signs and abstaining from intercourse during fertile periods when avoiding pregnancy.
Sympto-Thermal Method
The sympto-thermal method combines multiple ovulation indicators including basal body temperature, cervical mucus, and cycle length calculations. When used correctly, this method can be 95-99% effective for pregnancy avoidance.
Cervical Mucus Method
The Billings ovulation method focuses specifically on cervical mucus changes to identify fertile periods. Women learn to recognize mucus patterns that indicate approaching ovulation, peak fertility, and the return to infertility.
Modern Fertility Awareness
Contemporary fertility awareness methods integrate traditional techniques with modern technology including smartphone apps, digital thermometers, and hormone monitoring devices to improve accuracy and convenience.
Research and Future Developments
Molecular Understanding
Advanced research is revealing the molecular mechanisms controlling ovulation, including growth factors, inflammatory mediators, and genetic regulators of follicle development. This knowledge may lead to new therapeutic targets for ovulation disorders.
Biomarker Development
Scientists are developing new biomarkers for ovulation prediction and quality assessment, including anti-Müllerian hormone (AMH), inhibin B, and other markers that could improve fertility assessment and treatment.
Precision Medicine
Future approaches may include genetic testing to predict individual ovulation patterns, personalized hormone profiles, and customized fertility treatments based on individual reproductive characteristics.
Technology Integration
Emerging technologies including continuous hormone monitoring, artificial intelligence for cycle prediction, and integration with overall health tracking promise to revolutionize ovulation awareness and fertility management.
Frequently Asked Questions
How do I know when I’m ovulating?
Signs of ovulation include changes in cervical mucus (becoming clear and stretchy), mild pelvic pain (mittelschmerz), breast tenderness, and a slight temperature rise after ovulation. Ovulation predictor kits can detect the LH surge 12-36 hours before ovulation occurs.
Can you get pregnant outside of ovulation?
Pregnancy can only occur if sperm and egg meet, which requires ovulation. However, since sperm can survive up to 5 days in fertile cervical mucus, intercourse several days before ovulation can still result in pregnancy when ovulation occurs.
Why doesn’t ovulation happen on day 14 for everyone?
Only about 10% of women consistently ovulate on day 14. Normal ovulation can occur anywhere from day 11-21 in regular cycles, depending on individual cycle length and hormonal patterns. The key is that ovulation typically occurs 12-16 days before the next period.
Can stress affect ovulation timing?
Yes, acute or chronic stress can delay or prevent ovulation by disrupting the hormonal signals that control the menstrual cycle. Stress management techniques and addressing underlying stressors can help restore normal ovulation patterns.
How long does ovulation last?
The actual release of the egg from the follicle takes only a few minutes, but the ovulation process spans about 24 hours. The LH surge begins 12-36 hours before ovulation, and the egg remains viable for 12-24 hours after release.
Is it normal to feel pain during ovulation?
About 20% of women experience mittelschmerz (ovulation pain), which can range from mild twinges to more noticeable cramping. This pain is generally normal and results from follicle swelling and rupture, though severe pain should be evaluated medically.
Can you ovulate more than once per cycle?
Multiple ovulation can occur but must happen within the same 24-hour window. This can result in fraternal twins if both eggs are fertilized. True multiple ovulation events separated by days or weeks in the same cycle is extremely rare in humans.